RSS Feed
RSS Feed Twitter
Twitter 3:24 μ.μ.
3:24 μ.μ.
 Unknown
Unknown
ΟΣΦΥΑΛΓΙΑ ΚΑΙ ΣΤΗΡΙΞΗ ΣΤΑ ΠΕΛΜΑΤΑ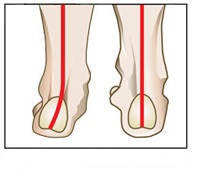
Όλοι οι ερευνητές συμφωνούν ότι η αρχιτεκτονική του άκρου πόδα σχετίζεται με την μορφολογία της λεκάνης, αλλά ένα ερώτημα που προκύπτει είναι: υπάρχει σύνδεση μεταξύ του τρόπου στήριξης στα πέλματα και την εμφάνιση οσφυαλγίας;
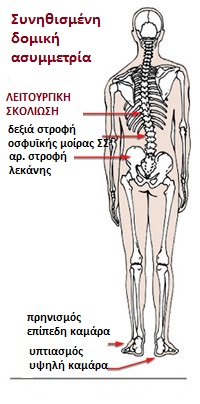
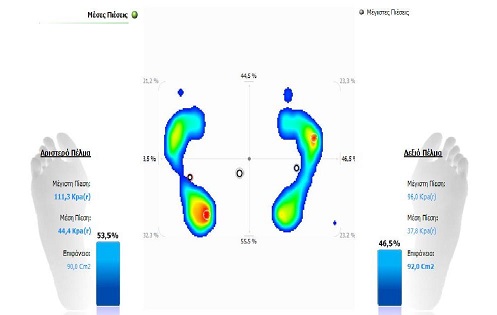
Ας υποθέσουμε ότι στην όρθια στάση ο αριστερός άκρος πόδας βρίσκεται σεπρηνισμό, που τυπικά προκαλείται από βλαισότητα στην υποστραγαλική άρθρωση (STJ), συνοδευόμενη από πτώση του σκαφοειδούς οστού. Ο δεξιός άκρο πόδας βρίσκεται σε υπτιασμό, όπου η υποστραγαλική άρθρωση είναι σε ραιβότητα, συνοδευόμενη από πτώση του κυβοειδούς οστού. Αυτός ο συνδυασμός πρηνισμού και υπτιασμού δεν επηρεάζει μόνο το φαινομενικό μήκος των ποδιών, αλλά ξεκινά μια μορφολογική διαταραχή που ταξιδεύει προς τα πάνω στην κινητική αλυσίδα, προκαλώντας στρέβλωση στο γόνατο, το ισχίο, τη λεκάνη και στις δομές της μέσης.
 Καθώς ο πρηνισμός στον αριστερό άκρο πόδα προκαλεί έσω στροφή στον μηρό, ενώ ο υπτιασμός στον δεξιό άκρο πόδα προκαλεί έξω στροφή στον μηρό, το άτομο θα ωθείτο να βαδίζει πλαγίως σε κάθε βήμα του. Φυσικά το ιδιοδεκτικό σύστημα του οργανισμού δεν μπορεί να επιτρέψει κάτι τέτοιο, οπότε κάνει προσαρμογές. Μια από αυτές τις προσαρμογές σχετίζεται με τη θέση της κεφαλής του μηριαίου οστού στη κοτύλη.
Καθώς ο πρηνισμός στον αριστερό άκρο πόδα προκαλεί έσω στροφή στον μηρό, ενώ ο υπτιασμός στον δεξιό άκρο πόδα προκαλεί έξω στροφή στον μηρό, το άτομο θα ωθείτο να βαδίζει πλαγίως σε κάθε βήμα του. Φυσικά το ιδιοδεκτικό σύστημα του οργανισμού δεν μπορεί να επιτρέψει κάτι τέτοιο, οπότε κάνει προσαρμογές. Μια από αυτές τις προσαρμογές σχετίζεται με τη θέση της κεφαλής του μηριαίου οστού στη κοτύλη.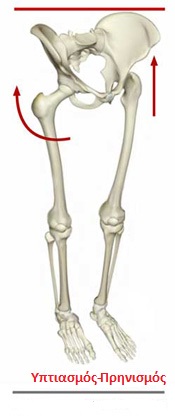 Στο αριστερό πόδι -που ο μηρός βρίσκεται σε έσω στροφή- ο αυχένας του μηριαίου οστού επίσης είναι σε έσω στροφή, γεγονός που ωθεί την κεφαλή προς τα πίσω ενάντια στην κοτύλη. Αντίθετα στο δεξιό πόδι -που ο μηρός βρίσκεται σε έξω στροφή- περιστρέφει τον αυχένα του μηριαίου, προκαλώντας ώθηση ενάντια στο πρόσθιο τμήμα της κοτύλης.
Στο αριστερό πόδι -που ο μηρός βρίσκεται σε έσω στροφή- ο αυχένας του μηριαίου οστού επίσης είναι σε έσω στροφή, γεγονός που ωθεί την κεφαλή προς τα πίσω ενάντια στην κοτύλη. Αντίθετα στο δεξιό πόδι -που ο μηρός βρίσκεται σε έξω στροφή- περιστρέφει τον αυχένα του μηριαίου, προκαλώντας ώθηση ενάντια στο πρόσθιο τμήμα της κοτύλης.Με τη δεξιά μηριαία κεφαλή να ωθεί προς τα εμπρός και την αριστερή προς τα πίσω, τα οστά της λεκάνης ωθούνται σε αριστερή στροφή. Αυτό συμβαίνει γιατί -καθώς η ανυψωμένη κεφαλή του μηριαίου δεξιά οδηγεί την πρόσθια λαγόνια ακρολοφία προς επάνω και πίσω, περιστρέφοντας τη λεκάνη-, αντισταθμιστικά, η αριστερή πλευρά βυθίζεται. Ως εκ τούτου προκαλείται ασύμμετρη στροφή της λεκάνης, με αποτέλεσμα το μπλοκάρισμα στην οσφυϊκή μοίρα της σπονδυλικής στήλης. Δεν πρέπει να ξεχνάμε ότι η λεκάνη είναι η βάση στήριξης της σπονδυλικής στήλης. Η ασυμμετρία της θα προκαλέσει την προσαρμογή της σπονδυλικής στήλης σε μια σκολιωτική στάση, που θα οδηγήσει σε υπολειτουργικότητα και μυϊκή ανισορροπία.
Επικεντρώνοντας ο θεραπευτής την προσοχή του στη αποκατάσταση της συμμετρίας στην λεκάνη θα έχει, στην καλύτερη περίπτωση, ένα προσωρινό αποτέλεσμα, αλλά δεν θα έχει αποκαταστήσει το πρόβλημα του ασθενή.
 Ο πρηνισμός και ο υπτιασμός στον άκρο πόδα όχι μόνο μπορούν να προκαλέσουν στροφή της λεκάνης, αλλά μπορούν να οδηγήσουν σε μια αντισταθμιστική σκολιωτική στάση την οσφυϊκή μοίρα της σπονδυλικής στήλης, μεταφέροντας το πρόβλημα προς τα πάνω στη θωρακική και αυχενική περιοχή. Ο θεραπευτής επιβάλλεται να έχει μια σφαιρική προσέγγιση κατά τη διάρκεια της κλινικής αξιολόγησης, ώστε να αναγνωρίσει τον μηχανισμό πίσω από το πρόβλημα του ασθενή.
Ο πρηνισμός και ο υπτιασμός στον άκρο πόδα όχι μόνο μπορούν να προκαλέσουν στροφή της λεκάνης, αλλά μπορούν να οδηγήσουν σε μια αντισταθμιστική σκολιωτική στάση την οσφυϊκή μοίρα της σπονδυλικής στήλης, μεταφέροντας το πρόβλημα προς τα πάνω στη θωρακική και αυχενική περιοχή. Ο θεραπευτής επιβάλλεται να έχει μια σφαιρική προσέγγιση κατά τη διάρκεια της κλινικής αξιολόγησης, ώστε να αναγνωρίσει τον μηχανισμό πίσω από το πρόβλημα του ασθενή.
Επίσης, πολλές φορές διαπιστώνουμε πρηνισμό και στους δυο άκρους πόδες, με αποτέλεσμα αυξημένη οσφυϊκή λόρδωση, αυξημένη οσφύοϊερή γωνία και 'φρακάρισμα' στις αρθρώσεις (facets) μεταξύ του 4ο οσφυϊκού με 5ο οσφυϊκό σπόνδυλο και 5ου οσφυϊκού με 1ο ιερό σπόνδυλο. Στους ασθενείς αυτούς και οι δυο μηριαίες κεφαλές είναι τοποθετημένες προς τα πίσω, με αποτέλεσμα η λεκάνη να ωθείτε προς τα εμπρός και να αυξάνεται η λόρδωση στην οσφυϊκή μοίρα. Το αντίθετο συμβαίνει στη περίπτωση όπου διαπιστώνουμε υπτιασμό και στους δυο άκρους πόδες. Τότε προκαλείται ευθειασμός στην οσφυϊκή μοίρα της σπονδυλικής στήλης.
Όπως πολύ πειστικά ανέφερε ο Sir William Osler: «Για να μπορέσουμε να θεραπεύσουμε κάτι, πρέπει πρώτα να είμαστε σε θέση να το αναγνωρίσουμε»
Βιβλιογραφία
1.
Zink G J. AN Osteopathic Structural Examination of the Soma. OsteopathicAnnals 7:12-19, 1979
2.
Previc F. A General Theory Concerning the Prenatal Origins of CerebralLateralizations in Humans. Psychological Review. Volume 98, 1991
3.
Geschwind N. Cerebral Lateralization. MIT Press, 1987
Zink G J. AN Osteopathic Structural Examination of the Soma. OsteopathicAnnals 7:12-19, 1979
2.
Previc F. A General Theory Concerning the Prenatal Origins of CerebralLateralizations in Humans. Psychological Review. Volume 98, 1991
3.
Geschwind N. Cerebral Lateralization. MIT Press, 1987


 • Λανθασμένη στάση κατά την διάρκεια της ξεκούρασης.
• Λανθασμένη στάση κατά την διάρκεια της ξεκούρασης.