ΑΞΙΟΛΟΓΗΣΗ ΝΕΥΡΟΛΟΓΙΚΩΝ ΣΥΜΠΤΩΜΑΤΩΝ
Κάποιος μπορεί να ισχυριστεί ότι η αξιολόγηση των νευρικών διαταραχών θα πρέπει να αφήνεται στο ιατρικό προσωπικό που έχει την σχετική εκπαίδευση, αλλά και πρόσβαση σε Μαγνητική αξονική τομογραφία, ηλεκτρομυογράφημα (ΗΜΓ) και άλλες διαγνωστικές δοκιμασίες. Αυτό είναι αλήθεια, αλλά η καθημερινή εμπειρία μας διδάσκει ότι οι περισσότεροι ιατροί στηρίζονται για καταλήξουν σε διάγνωση όλο και περισσότερο στις δίαφορες διαγνωστικές δοκιμασίες, αμελώντας τη κλινική αξιολόγηση. Εντούτοις, παρόλο που οι υψηλής τεχνολογίας διαγνωστικές μέθοδοι είναι σε αρκετές περιπτώσεις αποτελεσματικοί, δεν είναι πάντοτε ακριβής. Για παράδειγμα στο Μέσο Νεύρο δεν εντοπίζεται πάντοτε, κυρίως σε αρχικό στάδιο, το Σύνδρομο του Καρπιαίου Σωλήνα με το ΗΜΓ. Η κλινική νευρολογική αξιολόγηση έχει ένα υψηλό βαθμό αξιοπιστίας και θα πρέπει πάντοτε να είναι μέρος μιας αναλυτικής αξιολόγησης από τη μεριά του θεραπευτή.
Η εκτίμηση της λειτουργικότητας των αισθητικών νευρικών ινών σε σχέση με τις κινητικές, είναι σημαντικός παράγοντας όταν αξιολογούμε τα νευρολογικά συμπτώματα. Η πλειοψηφία των παθήσεων στα νεύρα επηρεάζουν τα περιφερειακά νεύρα.
Τα περιφερειακά νεύρα έχουν μια ραχιαία ρίζα που μεταφέρει αισθητικές πληροφορίες και μια κοιλιακή ρίζα που μεταφέρει κινητικές εντολές. Οι νευρικές ρίζες αναμιγνύονται μεταξύ τους λίγο μετά την έξοδο τους από τον Νωτιαίο Μυελό, συγκλίνουν στη δημιουργία των μεγάλων κορμών των περιφερειακών νεύρων, έχουν πορεία δια μέσου των άνω και κάτω άκρων, όπως και σε άλλες περιοχές του σώματος. Τα περισσότερα περιφερειακά νεύρα περιλαμβάνουν τόσο κινητικές, όσο και αισθητικές ίνες. Υπάρχουν όμως μερικά που είναι εφοδιασμένα με ίνες αισθητικές ή κινητικές σχεδόν αποκλειστικά.
Παθολογίες συμπίεσης είναι ο πιο κοινός τύπος τραυματισμού νεύρων. Η συμπίεση μπορεί να συμβεί οπουδήποτε στη διαδρομή κατά μήκος του νεύρου, από τη ρίζα του μέχρι το απώτερο άκρο του. Πίεση σε μια νευρική ρίζα ονομάζεται ριζοπάθεια. Παραδείγματα αποτελούν, η κήλη του μεσοσπονδυλίου δίσκου, όγκοι του νωτιαίου μυελού, τα οστεόφυτα και η σπονδυλική στένωση, τα οποία προκαλούν στένωση στο μεσοσπονδύλιο τρήμα, από όπου εξέρχεται η νευρική ρίζα από τη σπονδυλική στήλη.
Όταν ασκείτε πίεση σε ένα νεύρο κατά μήκος της πορείας του στα άνω ή κάτω άκρα, χαρακτηρίζεται περιφερειακή νευροπάθεια. Συνηθισμένα παραδείγματα περιφερειακής νευροπάθειας αποτελούν, το σύνδρομο του καρπιαίου σωλήνα, το σύνδρομο της θωρακικής εξόδου και το σύνδρομο του απιοειδούς μυός. Σε μια περιφερική νευροπάθεια, το νεύρο μπορεί να δεχθεί συμπίεση από τους μύες, ινώδεις ταινίες, οστά, τένοντες, τοπική φλεγμονή ή άλλους παράγοντες. Η θεραπεία επικεντρώνεται στην μείωση της συμπίεσης στο προσβεβλημένο νεύρο, άρα ο θεραπευτής πρέπει να μπορεί να αναγνωρίζει, όταν υπάρχει, αυτή την επιβλαβή συμπίεση.
ΑΞΙΟΛΟΓΗΣΗ ΣΥΜΠΤΩΜΑΤΩΝ
Είναι αναγκαία, για την επιλογή της πιο κατάλληλης θεραπευτικής στρατηγικής, η εκτίμηση της περιοχής και του τύπου της παθολογίας του νεύρου. Με την αξιολόγηση επιδιώκουμε τη συλλογή όσο το δυνατόν περισσοτέρων πληροφοριών για τα συμπτώματα του ασθενή. Το επιτυγχάνουμε με το λεπτομερές ιστορικό και τη κλινική αξιολόγηση.
Τα περισσότερα από τα μεγάλα περιφερικά νεύρα μεταφέρουν τόσο κινητικές, όσο και αισθητικές ίνες, οι οποίες παρουσιάζουν διαφορετικά πατέντα συμπτωμάτων. Κατά συνέπεια, όταν υπάρχει βλάβη στο νεύρο, μπορεί να υπάρχουν κινητικά ή αισθητικά συμπτώματα. Ωστόσο, ορισμένα νεύρα μεταφέρουν ένα πολύ μεγαλύτερο ποσοστό είτε κινητικών, είτε αισθητικών ινών. Σε αυτές τις περιπτώσεις, είναι πιο συχνό το πατέντο συμπτωμάτων των ινών που κυριαρχούν.
Για παράδειγμα, αν ο απιοειδής μυς παγιδεύσει το οπίσθιο μηριαίο δερματικό νεύρο στη περιοχή των γλουτών, τα συμπτώματα είναι πιο πιθανό να είναι πόνος ή παραισθησία στον οπίσθιο μηρό, επειδή αυτό το νεύρο είναι κυρίως ένα αισθητικό νεύρο που νευρώνει τον οπίσθιο μηρό. Αν ο απιοειδής μυς συμπιέσει το ανώτερο γλουτιαίο νεύρο, το πιο κοινό σύμπτωμα είναι αδυναμία στους απαγωγείς μύες του ισχίου, επειδή αυτό το νεύρο κυρίως είναι κινητικό νεύρο που νευρώνει τους απαγωγείς του ισχίου.
Τα πιο συνηθισμένα αισθητικά συμπτώματα από συμπίεση νεύρου είναι: πόνος, παραισθησία (μυρμηγκιάσματα), μούδιασμα, κάψιμο ή ηλεκτρικού τύπου αισθήσεις. Γίνονται αντιληπτά μακριά από τη περιοχή συμπίεσης. Βέβαια υπάρχουν εξαιρέσεις σε αυτή τη κατευθυντήρια γραμμή.
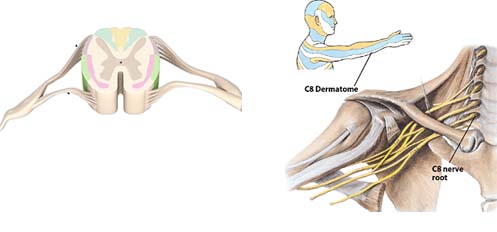
Τα συμπτώματα από τη συμπίεση νευρικής ρίζας είναι συνήθως διαφορετικά από εκείνα της συμπίεσης περιφερικού νεύρου. Η διάκριση αυτή έχει σημαντικές προεκτάσεις για τη θεραπεία. Όταν ασκείται πίεση σε μια νευρική ρίζα, τα συμπτώματα είναι αισθητά σε οποιοδήποτε σημείο εντός του συγκεκριμένου δερμοτομίου.
Δερμοτόμιο είναι μια περιοχή του δέρματος που νευρώνεται από μια συγκεκριμένη νευρική ρίζα. Ωστόσο αυτό δεν είναι απόλυτο, ούτε σε κάθε άνθρωπο είναι ακριβώς το ίδιο. Μπορεί να υπάρχουν μικρές αλλαγές στα δερμοτόμια λόγω ανατομικών ανωμαλιών. Σε ορισμένες περιπτώσεις τα συμπτώματα από πίεση στη νευρική ρίζα γίνονται αισθητά μόνο σε κάποιο τμήμα του δερμοτομίου, γεγονός που καθιστά δύσκολο να εντοπίσουμε το πρόβλημα.
Τα συμπτώματα από τη συμπίεση περιφερικού νεύρου γίνονται αντιληπτά σε περιοχές που υπερκαλύπτουν τα δερμοτόμια. Κάθε περιφερικό νεύρο παρέχει αισθητική νεύρωση σε μια συγκεκριμένη περιοχή του δέρματος στα άκρα, αυτό ονομάζεται δερματική νεύρωση του νεύρου. Για παράδειγμα, η δερματική νεύρωση του ωλένιου νεύρου περιορίζεται προς τη πλευρά της ωλένης του χεριού. Σαφώς υπάρχει επικάλυψη μεταξύ της δερματικής νεύρωσης του ωλένιου νεύρου και του Α8 δερμοτόμιου. Τέτοιες επικαλύψεις κάνουν τη κλινική ανάλυση πιο προκλητική.
Άρα πως θα αντιληφθούμε την προέλευση των συμπτωμάτων;
Θα το επιτύχουμε μέσα από μια πιο ακριβή και λεπτομερή αξιολόγηση. Γενικά όμως αν τα συμπτώματα γίνονται αντιληπτά σε ολόκληρη την έκταση του δερμοτομίου, τότε πιθανώς έχουμε πρόβλημα νευρικής ρίζας (ριζοπάθεια). Αν τα συμπτώματα περιορίζονται σε δερματική νεύρωση ενός νεύρου, τότε πρόκειται για περιφερική νευροπάθεια. Για παράδειγμα, εάν ο ασθενής παρουσιάσει συμπτώματα κατά μήκος της έσω πλευρά του βραχίονα και του πήχη με επέκταση στο χέρι, στο Α8 δερμοτόμιο δηλαδή, τότε θεωρούμε ότι υπάρχει ριζοπάθεια. Εάν τα συμπτώματα είναι αισθητά μόνο στη πλευρά της ωλένης του χεριού, τότε πιθανόν πρόκειται για πίεση κάπου κατά μήκος του ωλένιου νεύρου περιφερικά. Όμως λόγω της επικάλυψης μεταξύ του δερμοτόμιου και της δερματικής νεύρωσης, περαιτέρω έλεγχος θα είναι δικαιολογημένος. Επιπλέον περαιτέρω δοκιμές θα χρειαστούν γα να προσδιοριστεί ακριβώς η θέση της πίεσης κατά μήκος της διαδρομής του νεύρου, ώστε να καθοριστεί η θεραπευτική προσέγγιση.
Κατά την νευρολογική αξιολόγηση, δεν πρέπει πάντα να υποθέτουμε πώς υπάρχει μηχανικό πρόβλημα συμπίεσης. Πολλές συστηματικές διαταραχές, όπως η μυασθένεια Gravis ή ο διαβήτης μπορούν να προκαλέσουν περιφερικά νευρολογικά συμπτώματα, όπως επίσης μπορούν τα μυοπεριτοναϊκά σημεία πυροδότησης πόνου (trigger points), κ.α. Η διαφορική διάγνωση είναι απαραίτητη.
Οι παθήσεις των νεύρων επηρεάζουν την κινητική λειτουργία όταν εμπλέκονται οι κινητικές ίνες. Το πιο κοινό σύμπτωμα από τη συμπίεση των κινητικών νεύρων είναι η αδυναμία και ατροφία των μυών που νευρώνονται από το προσβεβλημένο νεύρο. Όπως και με τις αισθητικές διαταραχές, οι πληγέντες μύες είναι απομακρυσμένοι από το σημείο συμπίεσης. Κατά συνέπεια, όσο απομακρυνόμαστε από το σημείο συμπίεσης, τόσο λιγότεροι είναι οι πληγέντες μύες.
Στο σχήμα βλέπουμε μια σχηματική συμπίεση δύο σημείων στη πορεία ενός νεύρου και πως αυτή επηρεάζει τους μύες που νευρώνονται από αυτό.
Η μυϊκή αδυναμία και η ατροφία είναι τα πιο εμφανή συμπτώματα από τη συμπίεση των κινητικών νεύρων. Ωστόσο, σε μερικές περιπτώσεις η παθολογία προκύπτει από τη μεταβολή των βιομηχανικών πατέντων, ως αποτέλεσμα της μυϊκής αδυναμίας, λόγω του τραυματισμού του νεύρου. Οι περισσότερες κινήσεις μας περιλαμβάνουν πολύπλοκα σχήματα συντονισμού ενός συνόλου μυών για να επιτευχθεί μια εργασία. Η αδυναμία ή ατροφία ενός ή περισσότερων μυών προκαλεί συνεπακόλουθα προβλήματα που μπορεί από πρώτη ματιά να μη φαίνονται σχετικά με το πρόβλημα.
Για παράδειγμα, το μακρύ θωρακικό νεύρο νευρώνει τον πρόσθιο οδοντωτό μυ, που είναι σημαντικός στη κίνηση της ωμοπλάτης κατά την απαγωγή του ώμου. Σπασμός στον σκαληνό μυ, μπορεί να συμπιέσει το μακρύ θωρακικό νεύρο και να προκαλέσει αδυναμία στον πρόσθιο οδοντωτό μυ. Επίσης, μεταφέροντας ένα σακίδιο ή άλλο βαρύ αντικείμενο με ιμάντα ώμου, θα μπορούσε να προκληθεί συμπίεση του νεύρου. Σε αδυναμία του πρόσθιου οδοντωτού μυ, διαταράσσεται ο συντονισμός των κινήσεων μεταξύ της ωμοπλάτης και του βραχιονίου οστού στην απαγωγή του ώμου, που μπορεί να οδηγήσει σε σύνδρομο πρόσκρουσης. Μπορεί να μη σκεφτούμε τη συμπίεση νεύρου, ως βασική αιτία του προβλήματος, αλλά η μυϊκή αδυναμία ως αποτέλεσμα της συμπίεσης είναι η ρίζα του προβλήματος.
Όλο και περισσότεροι φυσικοθεραπευτές σήμερα εργάζονται με ασθενείς/πελάτες που παρουσιάζουν μια διευρυμένη ποικιλία συμπτωμάτων πόνου και τραυματικών καταστάσεων. Είναι ζωτικό να μπορούν να αντιληφθούν πότε τα συμπτώματα προέρχονται από τα νεύρα. Σε κάποιες περιπτώσεις, ο ασθενής πρέπει να παραπέμπεται σε κάποιο άλλο επαγγελματία υγείας για περαιτέρω αξιολόγηση, κυρίως αν το συγκεκριμένο πρόβλημα του ασθενή ξεπερνά τις δυνατότητες του θεραπευτή ή δεν βρίσκεται στο φάσμα των επαγγελματικών του δυνατοτήτων.
Σε όλες τις περιπτώσεις όμως απαιτείται η κατάλληλη και επαρκή εκπαίδευση των φυσικοθεραπευτών, ώστε να μπορούν να ανταποκριθούν στις καθημερινές προκλήσεις που καλούνται να αντιμετωπίσουν, προς όφελος των ασθενών τους.
ΒΙΒΛΙΟΓΡΑΦΙΑ:
1-Boden SD, Davis DO, Dina TS, et al. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990;72(3):403-8.
2-Borenstein DG, O'Mara JW, Jr., Boden SD, et al. The value of magnetic resonance imaging of the lumbar spine to predict low back pain in asymptomatic subjects: a seven-year follow-up study. J Bone Joint Surg Am 2001;83-A(9):1306-11.
3-Jensen MC, Brant-Zawadzki MN, Obuchowski N, et al. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 1994;331(2):69-73.
4-Schmid AB, Brunner F, Luomajoki H, et al. Reliability of clinical tests to evaluate nerve function and mechanosensitivity of the upper limb peripheral nervous system. BMC Musculoskelet Disord 2009;10:11.
πηγη http://physio.gr/
 RSS Feed
RSS Feed Twitter
Twitter 3:49 μ.μ.
3:49 μ.μ.
 Unknown
Unknown






















